Endari (L-glutamine) for sickle cell disease
Last updated May 30, 2024, by Andrea Lobo, PhD
 Fact-checked by Inês Martins, PhD
Fact-checked by Inês Martins, PhD
What is Endari for sickle cell disease?
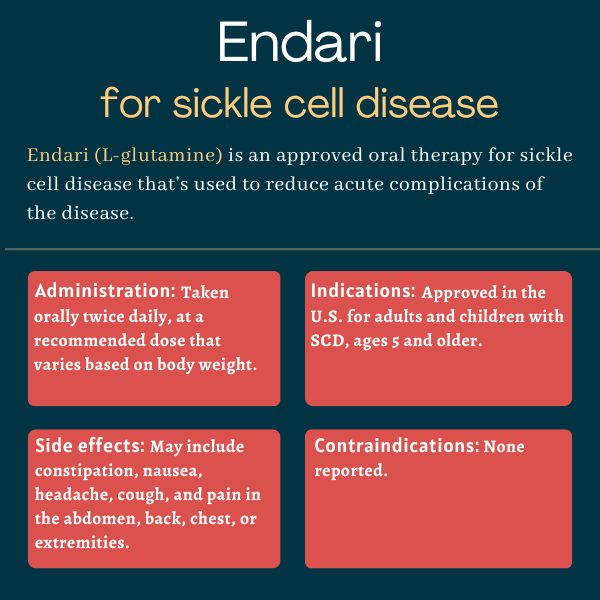
Endari (L-glutamine) is an oral therapy approved in the U.S. for children and adults with sickle cell disease (SCD), ages 5 and older. It’s used to reduce acute disease complications such as pain crises.
Developed by Emmaus Life Sciences, it’s available as an oral powder that’s dissolved in a liquid or soft food before administering.
Therapy snapshot
| Brand name: | Endari |
| Chemical name: | L-glutamine |
| Usage: | Used to reduce acute complications of sickle cell disease |
| Administration: | Oral powder |
How does Endari work?
Sickle cell disease is caused by mutations in the HBB gene, which leads to the production of a faulty version of hemoglobin, the protein in red blood cells responsible for transporting oxygen, called hemoglobin S. Hemoglobin S tends to clump up inside red blood cells, causing them to acquire the sickle-like shape that marks the disease.
While normal red blood cells are round and flexible, letting them easily move through small blood vessels, the misshapen red blood cells are rigid and prone to stick to each other. This can block blood flow and lead to a shortage of oxygen in several tissues, which may cause acute pain crises, known as vaso-occlusive crises (VOCs).
Red blood cells in sickle cell disease are also more fragile and die prematurely, leading to a constant shortage of red blood cells, called anemia.
One reason why sickled red blood cells become sticky and are prone to die prematurely is their increased susceptibility to oxidative stress, a type of cellular damage caused by an excess of free radicals that can’t be properly detoxified by the cells’ antioxidant defenses.
Endari is made to boost antioxidant production to help curb oxidative damage in red blood cells. It contains the amino acid L-glutamine, which is needed to build out proteins, but can also be used by sickled cells to produce antioxidant molecules.
By helping to neutralize oxidative stress, these antioxidants let red blood cells regain their flexibility, enabling them to travel more smoothly through blood vessels and carry oxygen to tissues throughout the body.
For this reason, Endari should reduce acute disease complications, including pain crises and hospital admissions, in people with SCD.
Who can take Endari?
Endari was approved by the U.S. Food and Drug Administration (FDA) in July 2017 for SCD patients, ages 5 and older. The decision made Endari the first approved treatment for children with SCD and the first new treatment for adults with the disease in almost 20 years.
Emmaus also submitted an application to the European Medicines Agency to seek the medication’s approval in the European Union, where it would have been sold as Xyndari. The company withdrew its application in 2019 after an advisory committee recommended against approving the therapy, however.
The company has since received scientific advice from the committee, but it’s not clear if it plans to resubmit in the future.
Who should not take Endari?
The prescribing information for Endari lists no contraindications or warnings associated with its use in people with SCD.
How is Endari administered?
Endari is available as paper-foil-plastic laminate packets, each containing 5 g of a L-glutamine white crystalline powder.
The medication is taken orally twice a day — once in the morning and once in the evening — at recommended doses that vary by weight. They are:
- one packet per dose, or two daily packets, for patients weighing less than 30 kg (66 lbs)
- two packets per dose, or four daily packets, for patients weighing between 30 and 65 kg (66-143 lbs)
- three packets per dose, or six daily packets, for patients weighing more than 65 kg (over 143 lbs)
Immediately before ingestion, the contents of each packet should be mixed with eight ounces (240 mL, or one full cup) of a cold or room temperature beverage, such as water, milk, or apple juice. It can also be mixed with 4-6 ounces of soft foods such as applesauce or yogurt. Complete dissolution is not required before administering.
If a dose is missed, it should be taken as soon as possible. Patients should not double their dose to make up for a missed one.
Endari in clinical trials
Endari’s safety and efficacy were evaluated mainly in two clinical trials, a Phase 2 trial (NCT00125788) and a Phase 3 trial (NCT01179217). Both enrolled people ages 5 and older with either SCD or sickle beta 0 thalassemia, a related condition wherein red blood cells also carry the abnormal hemoglobin S but are small and pale, who’ve had at least two episodes of painful crises in the previous year.
Results from the Phase 3 study supported the approval of Endari for SCD.
Phase 2 trial
The Phase 2 study, launched in 2024, enrolled 81 people with SCD or sickle beta 0 thalassemia who were randomly assigned to receive either Endari or a placebo for 48 weeks, or nearly a year. Endari was given twice daily, at 0.3 g/kg per dose, adjusted to the nearest 10, 20, or 30 grams a day.
The trial’s main goal was to see if Endari could reduce the frequency of painful sickle cell crises compared with a placebo. Results showed the average number of painful crises per patient was much lower with Endari, both after six months (2.5 vs. 5.5) and one year (4.5 vs. 10.8). The differences weren’t statistically significant, however.
The mean number of hospitalizations and emergency room visits due to sickle cell pain also decreased with Endari after six months and one year, although only the frequency of hospitalizations after six months was significantly different from the placebo group (0.8 vs. 1.3).
The therapy was also well tolerated, with the frequency of side effects being similar in the Endari and placebo groups. The most commonly reported adverse effects were moderate to severe and were related to SCD crises. One death was reported, but was determined to be unrelated to the treatment.
Phase 3 trial
The pivotal Phase 3 trial enrolled 230 SCD or sickle beta 0 thalassemia patients who randomly received twice daily Endari (0.3 g/kg per dose, also adjusted to 10, 20, or 30 g per day) or a placebo for 48 weeks. About two-thirds of the patients in each group also received the standard SCD treatment hydroxyurea.
Nearly one year of treatment with Endari significantly reduced the number of pain crises by 25% compared with the placebo (median, 3 vs. 4). There were also fewer episodes of acute chest syndrome, a serious lung condition that causes fever, chest pain, and breathing problems, with Endari, with 8.6% of patients in this group having at least one episode, versus 23.1% in the placebo group.
The Endari group also saw a significant, 33% decrease in hospitalization rates (median, 2 vs. 3), and spent significantly fewer days in the hospital (6.5 vs. 11). The number of emergency department visits that didn’t result in hospitalization, however, wasn’t significantly different between the groups.
Regarding safety, the patients given Endari had lower rates of side effects and serious side effects than those on a placebo. Still, five patients withdrew from the trial due to side effects and two patients with a long history of organ failure died of sudden cardiac death.
Common side effects of Endari
The most common side effects of Endari reported in clinical trials include:
- constipation
- nausea
- headache
- abdominal pain
- cough
- pain in the extremities, back, and/or chest.
Use in pregnancy and breastfeeding
There are no available preclinical or clinical data to determine whether Endari can cause damage to a developing fetus or affect reproductive capacity in women. It’s also not known if Endai can be found in human milk, or whether it has any negative effects on milk production or on a nursing child.
Patients who are pregnant or planning to become pregnant and those who are breastfeeding should talk with their doctor and consider the potential risks and benefits of taking the medication in these situations.
Sickle Cell Disease News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Related articles
-
-
 Discussion
Discussion
-
-

-

-