
 Fact-checked by
Fact-checked by 
Lyfgenia (lovotibeglogene autotemcel) for sickle cell disease
What is Lyfgenia for sickle cell disease?
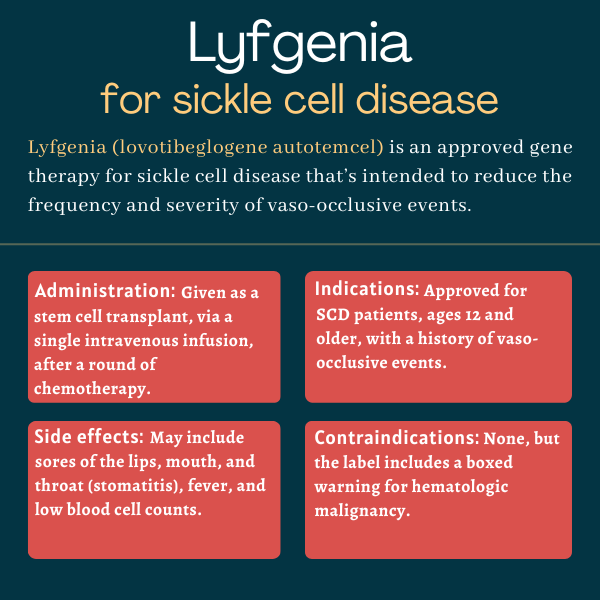
Lyfgenia (lovotibeglogene autotemcel), formerly known as LentiGlobin or lovo-cel, is a one-time gene therapy approved for people with sickle cell disease (SCD) with a history of vaso-occlusive events, known as VOEs.
It’s designed to reduce the frequency and severity of these events, which include painful vaso-occlusive crises (VOCs), acute chest syndrome, and other sickle cell-related complications.
The therapy, administered via a single intravenous or into-the-vein infusion, was developed by Bluebird Bio.
Therapy snapshot
| Brand name: | Lyfgenia |
| Chemical name: | Lovotibeglogene autotemcel |
| Usage: | Used to reduce the frequency and severity of vaso-occlusive events in sickle cell disease |
| Administration: | Intravenous infusion |
How does Lyfgenia work?
In sickle cell disease, known as SCD for short, a faulty version of hemoglobin — the protein that helps red blood cells carry oxygen — is produced due to mutations in the HBB gene. This abnormal form of hemoglobin, called hemoglobin S, is prone to clumping, causing red blood cells to take on a sickle-like shape that makes them rigid, sticky, and more prone to get stuck within blood vessels. This in turn can restrict blood flow and compromise oxygen transport in the body, leading to VOCs.
Lyfgenia is a gene therapy designed to provide patients with a modified HBB gene capable of producing a form of hemoglobin, called HbAT87Q, with anti-sickling properties. The gene is inserted into patients’ own hematopoietic stem cells, which serve as precursors to all mature blood cells in the body.
This enables red blood cells produced from these stem cells to be resistant to sickling, leading to fewer VOCs and other sickle cell complications. The modified gene is packaged into a lentivirus carrier that helps the therapy be taken up by a person’s cells.
The treatment involves collecting a patient’s hematopoietic stem cells and then treating them in the lab with the gene therapy. The cells than are returned to the patient via a stem cell transplant. A round of chemotherapy prior to the transplant eliminates unhealthy blood cells and makes room for the modified ones. The new stem cells will work to repopulate the blood with healthy hemoglobin-producing red blood cells.
Who can take Lyfgenia?
Lyfgenia was approved by the U.S. Food and Drug Administration in December 2023 for the treatment of SCD patients, ages 12 and older, with a history of VOEs.
Who should not take Lyfgenia?
No contraindications are listed in Lyfgenia’s prescribing information.
However, the therapy comes with a boxed warning noting that some patients who received treatment with an earlier version of Lyfgenia developed a blood cancer known as hematologic malignancy. Those receiving the gene therapy should be on lifelong monitoring for such cancers.
How is Lyfgenia administered?
Lyfgenia is manufactured specifically for each of its recipients using the patient’s own cells. This means there are several steps involved in obtaining a person’s cells, modifying them, and returning them to the body. This process can only be conducted at a qualified treatment center with the expertise to administer the therapy.
Prior to beginning the procedure, a healthcare team will confirm that the patient is eligible for a stem cell transplant. That requires that the patient has tested negative for human immunodeficiency virus (HIV) types 1 and 2. The patient also will receive at least two cycles of blood transfusions prior to stem cell collection to help keep hemoglobin levels high enough.
The individual receiving Lyfgenia also may need to stop using certain SCD medications for a period of time before beginning the treatment process. This will be determined by the patient’s healthcare team.
Stem cell collection and manufacturing
To obtain hematopoietic stem cells to make Lyfgenia, patients first will be treated with a medication called plerixafor, given as a liquid that’s injected subcutaneously, or under the skin. It mobilizes stem cells, causing them to move from the bone marrow where they reside into the bloodstream. Then, these cells are collected from the blood using a method called apheresis, which is done in a lab.
This cell collection process usually will be repeated for two consecutive days. If not enough cells are collected during the first session, another round may be conducted. This typically is done at least two weeks later, after the body has had time to make more stem cells. In most patients, the minimum number of cells required to manufacture Lyfgenia is obtained in one or two rounds, each with two collection days.
Some of the collected cells will be frozen and left unmodified as a backup, in case the individual needs a rescue stem cell transplant. The rest will be sent to a lab, where they will be treated with the gene therapy. A cell suspension of the modified cells will then be frozen in infusion bags and sent to the patient’s healthcare provider.
The entire process from stem cell collection to Lyfgenia being shipped to the patient’s healthcare provider takes about 10-15 weeks, though the length of time may vary.
After stem cell collection, additional medication modifications and blood transfusions may be required at the discretion of a healthcare provider before moving on to the next stage.
Myeloablative conditioning
Once Lyfgenia has been manufactured and is stored at the chosen healthcare center, patients will be admitted to their treatment center. Patients will remain at the center until after they receive Lyfgenia.
First, patients must undergo high-dose chemotherapy with an agent called busulfan to eliminate unhealthy blood stem cells and make room for the new ones in the bone marrow. Busulfan is given via an infusion directly into the bloodstream.
This process, known as myeloablative conditioning, will occur over four consecutive days and must be completed a minimum of two days prior to Lyfgenia administration. Preventive anti-seizure medications also may be given to patients before myeloablative conditioning starts.
Lyfgenia administration
At least two days after myeloablative conditioning, the Lyfgenia will be thawed and prepared by a healthcare provider, then administered via a stem cell transplant as an intravenous or into-the-vein infusion. Lyfgenia will be given at a weight-based dose; the minimum recommended dose is 3 million cells per kilogram of body weight.
The number of infusion bags needed to achieve this dose depends on the number of cells in each bag, which may vary from patient to patient. Patients will receive anywhere from one to four infusion bags, with each bag taking less than 30 minutes to infuse.
After receiving Lyfgenia, patients will stay at the treatment center for about 3-6 weeks so they can be closely monitored. Their healthcare providers will advise them on when they can go home, and also on which of their existing medications are safe to take — and when — after receiving Lyfgenia.
Lyfgenia in clinical trials
Lyfgenia is being evaluated in two ongoing open-label clinical trials — meaning that both participants and clinicians know the exact dose of the medication being given.
HGB-206 and HGB-210 trials
The Phase 1/2 HGB-206 trial (NCT02140554), which largely formed the basis of Bluebird’s regulatory application to the FDA, enrolled 54 patients with severe SCD. The participants, ages 12-50, were treated at sites in the U.S. All had experienced at least four severe VOEs in the two years prior to enrolling in the study. A total of 36 patients were given the gene therapy.
The trial’s main goal is to evaluate the proportion of patients who are completely free of VOEs in the 6-18 months after receiving Lyfgenia. VOEs include episodes of acute pain (VOCs) — lasting more than two hours and deemed to be caused by blood vessel blockage — acute chest syndrome, and other sickle cell-related complications requiring evaluation at a medical facility.
Trial data submitted to the FDA indicated that 28 of 32 evaluable patients (88.2%) saw a complete resolution of VOEs, and 30 (94%) did not experience any severe VOEs. Severe VOEs included those that required hospitalization, or multiple visits to urgent care over a period of three days, as well as intravenous treatment on each visit. Such events also included episodes of priapism, or painful erection, that required any level of medical attention.
Participants are continuing to be monitored, with an expected trial completion in 2024.
The Phase 3 HGB-210 trial (NCT04293185) is recruiting up to 35 SCD patients, ages 2-50, at sites in eight U.S. states plus the District of Columbia. As in the HGB-206 trial, participants will be monitored for the occurrence of VOEs in the 6-18 months after receiving the gene therapy. The trial is expected to finish in 2027.
The most recent update from Bluebird Bio concerned 34 of 47 patients who had received the gene therapy in either of the two trials. They had been followed for a median of 36.3 months, or about three years.
Data indicated that 94% of the patients experienced a resolution of severe VOEs, and 88.2% did not experience any VOEs over a median of 35.8 months, or just shy of the three-year mark. Among the eight patients who experienced VOEs at any time after receiving Lyfgenia, the frequency and severity of such events were significantly reduced compared with before treatment. In fact, all achieved a reduction in VOEs by at least 50%, and hospital stays and admissions per year were reduced by a median of 85.5%.
Measures of hemoglobin and red blood cell counts also were improved after treatment, as were measures of health-related quality of life. Most side effects were attributed to busulfan or underlying sickle cell disease.
Other ongoing trials
Bluebird also is sponsoring an observational study, called LTF-307 (NCT04628585), that will monitor the long-term safety and efficacy of Lyfgenia. It will involve patients given the therapy in other studies sponsored by the company, for a total of 15 years. This long-term study is expected to conclude in 2038.
Common side effects of Lyfgenia
On the day of Lyfgenia infusion, patients may experience infusion-related reactions such as low blood pressure and hot flushes.
Following treatment, the most common side effects reported in clinical trials of Lyfgenia include:
- inflamed and sore mouth, known as stomatitis
- fever due to low counts of immune cells called neutrophils
- low blood cell counts, including platelets, red blood cells, and white blood cells.
Blood cancer
Lyfgenia comes with a boxed warning for a risk of blood cancer, or hematologic malignancy, which has occurred in patients treated with previous versions of the gene therapy. SCD patients are also generally at a higher risk of developing blood cancer than are people in the general population.
This increased cancer risk could arise from cellular stress associated with stem cell mobilization, conditioning, or Lyfgenia infusion, including the need to repopulate the blood with new cells. Moreover, Lyfgenia could possibly cause insertional oncogenesis, in which genetic material is inserted in unwanted places of the genetic code. This causes gene activity changes that drive uncontrolled cell growth, promoting cancer development.
Patients should be closely monitored for signs of such cancers at least every six months, and for a minimum of 15 years after receiving the therapy. An integration site analysis, which looks at where genetic material has been inserted in the genetic code of a person’s cells, also should be conducted after six months and a year.
Blood cancer may cause no symptoms or generic symptoms. Patients should contact their healthcare providers right away if they experience symptoms such as abnormal bruising or bleeding, blood in the urine, stool, or vomit, coughing up blood, severe headache, unusual stomach or back pain, fever, swollen glands, or abnormal tiredness. If a person is diagnosed with cancer, the treating physician should report it to Bluebird Bio at 1-833-999-6378.
Changes in blood cell counts
A successful stem cell transplant depends on the new stem cells engrafting — implanting and multiplying — in the bone marrow in order to supply the body with new blood cells. It is possible that this process may be delayed or fail for certain types of blood cells after Lyfgenia treatment, leading to reduced blood cell counts.
Delays in the engraftment of platelets — small cell fragments involved in blood clotting — have been observed, which may cause platelet deficiencies, known as thrombocytopenia, and increase the risk of bleeding. Blood platelet counts should be checked until platelet engraftment is achieved. Blood tests should be conducted if clinical symptoms suggestive of bleeding are evident.
There also is a risk of an engraftment failure for neutrophils, a type of white blood cell or immune cell involved in the body’s response to infections. Neutrophil deficiency, or neutropenia, can increase the risk of infection. Neutrophil counts should be monitored until engraftment has been achieved. If engraftment fails, patients should be treated with a stem cell transplant using the backup, unmodified cells.
Allergic reactions
Allergic or hypersensitivity reactions may occur with Lyfgenia. Certain ingredients used to preserve Lyfgenia, including dimethyl sulfoxide and dextran 40, can cause hypersensitivity reactions, including a life-threatening type called anaphylaxis.
Use of other medications
Patients should not take preventive HIV anti-retroviral medications for at least a month prior to stem cell mobilization and until all stem cell collection cycles are finished. Some long-acting anti-retroviral agents may need to be stopped sooner. If a patient is using these medications, a negative test for HIV must be obtained prior to stem cell collection. The viral carrier used in Lyfgenia may cause a false positive on an HIV test using polymerase chain reaction (PCR) technology. Treated patients should not be screened for HIV via this detection method.
Hydroxyurea, an approved SCD therapy, should not be used by patients for at least two months before stem cell mobilization and until all stem cell collection cycles are completed. If hydroxyurea is restarted between stem cell collection and myeoloablative conditioning, it should be stopped again two days before the conditioning regimen.
Iron chelator treatments, which are generally used to treat iron overload that can occur in patients frequently receiving blood transfusions, should be stopped at least a week before stem cell collection. Myelosuppressive iron chelators, which are bone marrow-suppressing, should not be used for six months after Lyfgenia administration. Non-myelosuppressive iron chelators should not be restarted sooner than three months after the treatment.
Use in pregnancy and breastfeeding
There are no available data on the use of Lyfgenia during pregnancy or breastfeeding. It is not known whether Lyfgenia can be transferred to a developing fetus, and if so, what effects it will have. Likewise, it is not known if Lyfgenia passes into human breastmilk. Myeloablative conditioning, however, is associated with known risks during pregnancy and breastfeeding.
As such, Lyfgenia is not recommended for women who are pregnant or breastfeeding. A negative blood pregnancy test is required prior to the start of stem cell collection; the results must be reconfirmed prior to myeloablative conditioning and Lyfgenia administration.
Both male and female patients should use an effective method of contraception from the start of stem cell mobilization until at least six months after receiving Lyfgenia. Women who wish to become pregnant or breastfeed after receiving Lyfgenia should discuss this with their healthcare providers.
There are no data on whether Lyfgenia impacts fertility, but myeloablative conditioning does raise the risk of infertility. Patients should talk with their healthcare team about these risks and their options for fertility preservation prior to undergoing treatment.
Sickle Cell Disease News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Related articles
-
-

-

-
-
 Discussion
Discussion
-
